

CathrynCathryn Jakobson Ramin’s back pain started when she was 16, on the day she flew off her horse and landed on her right hip.
For the next four decades, Ramin says her back pain was like a small rodent nibbling at the base of her spine. The aching left her bedridden on some days and made it difficult to work, run a household, and raise her two boys.
By 2008, after Ramin had exhausted what seemed like all her options, she elected to have a “minimally invasive” nerve decompression procedure. But the $8,000 operation didn’t fix her back, either. The same pain remained, along with new neck aches.





At that point, Ramin decided to deploy her skills as a journalist and investigate the $100 billion back pain industry. She went on to write Crooked: Outwitting the Back Pain Industry and Getting on the Road to Recovery, an incredible tale of back pain and its treatment, published last May.
The big takeaway: Millions of back patients like Ramin are floundering in a medical system that isn’t equipped to help them. They’re pushed toward intrusive, addictive, expensive interventions that often fail or can even harm them, and away from things like yoga or psychotherapy, which actually seem to help. Meanwhile, Americans and their doctors have come to expect cures for everything — and back pain is one of those nearly universal ailments with no cure. Patients and taxpayers wind up paying the price for this failure, both in dollars and in health.
Thankfully, Ramin finally discovered an exercise program that has eased her discomfort. And to this day, no matter how busy her life gets, she does a series of exercises every morning called “the McGill Big Three” (more on them later). “With very rare exceptions,” she says, “I find time to exercise, even when I’m on the road.”
More and more people like Ramin are seeking out conservative therapies for back pain. While yoga, massage, and psychotherapy have been around for a long time, there was little high-quality research out there to understand their effects on back pain, and doctors sometimes looked down on these practices. But over the past decade, that’s changed.
To learn more, I searched the medical literature on treatments for lower back pain (the most common type) and read through more than 80 studies (mainly reviews of the research that summarized the findings of hundreds more studies) about both “active” approaches (yoga, Pilates, tai chi, etc.) and passive therapies (massage, chiropractics, acupuncture, and so on). I also talked to nine experts and researchers in this field. (For more detail on our methods, scroll to the end.)
What I found surprised me: Many of these approaches really do seem to help, though often with modest effects. But when you compare even those small benefits with the harm we’re currently doing while medically “treating” back pain, the horror of the status quo becomes clear. “No one dies of low back pain,” one back pain expert, University of Amsterdam assistant professor Sidney Rubinstein, summed up, “but people are now dying from the treatment.”
Mainstream medicine has failed people with chronic back pain
Lower back pain is one of the top reasons people go to the doctor in the US, and it affects 29 percent of adult Americans, according to surveys. It’s also the leading reason for missing work anywhere in the world. The US spends approximately $90 billion a year on back pain — more than the annual expenditures on high blood pressure, pregnancy and postpartum care, and depression — and that doesn’t include the estimated $10 to $20 billion in lost productivity related to back pain.
Doctors talk about back pain in a few different ways, but the kind most people (about 85 percent) suffer from is what they call “nonspecific low back pain.” This means the persistent pain has no detectable cause — like a tumor, pinched nerve, infection, or cauda equina syndrome.
About 90 percent of the time, low back pain is short-lived (or in medical lingo, “acute”) and goes away within a few days or weeks without much fuss. A minority of patients, though, go on to have subacute back pain (lasting between four and 12 weeks) or chronic back pain (lasting 12 or more weeks).
Chronic nonspecific back pain is the kind the medical community is often terrible at treating. Many of the most popular treatments on offer from doctors for chronic nonspecific low back pain — bed rest, spinal surgery, opioid painkillers, steroid injections — have been proven ineffective in the majority of cases, and sometimes downright harmful.
Consider opioids. As of 2016, 14,500 Americans died from opioid-related deaths. Opioid prescribing is common among people with back pain, with almost 20 percent receiving long-term opioid prescriptions.
Here’s the outrageous part: All these opioids were being prescribed before we actually knew if they helped people with chronic lower back pain. It gets worse: Now high-quality evidence is coming in, and opioids don’t actually help many patients with chronic low back pain.
This newly published randomized controlled trial was the first to compare the long-term use of opioids versus non-opioid medications (such as anti-inflammatory drugs and acetaminophen) for chronic low back pain, and hip or knee osteoarthritis. After a year, the researchers found opioids did not improve patients’ function any more than the non-opioids, and the patients on opioids were actually in slightly more pain compared to the non-opioid group (perhaps the result of “opioid-induced hyperalgesia” — heightened pain brought on by these drugs).
As for surgery, only a small minority of patients with chronic low back pain require it, according to UpToDate, a service that synthesizes the best available research for clinicians. In randomized trials, there was no clinically meaningful difference when comparing the outcomes of patients who got spinal fusion (which has become more and more popular in the US over the years) with those who got a nonsurgical treatment.
Steroid injections for back pain, another popular medical treatment, tend to have similarly lackluster results: They improve pain slightly in the short term, but the effects dissipate within a few months. They also don’t improve patients’ long-term health outcomes.
It’s not entirely surprising that the surgeries, injections, and prescription drugs often fail considering what researchers are now learning about back pain.
Historically, the medical community thought back pain (and pain in general) was correlated to the nature and severity of an injury or anatomical issue. But now it’s clear that what’s going on in your brain matters too.
“Our best understanding of low back pain is that it is a complex, biopsychosocial condition — meaning that biological aspects like structural or anatomical causes play some role but psychological and social factors also play a big role,” Roger Chou, a back pain expert and professor at Oregon Health and Science University, summarized.
For example, when you compare people with the same MRI results showing the same back injury — bulging discs, say, or facet joint arthritis — some may experience terrible chronic pain while others report no pain at all. And people who are under stress, or prone to depression, catastrophizing, and anxiety tend to suffer more, as do those who have histories of trauma in their early lives or poor job satisfaction.
The awareness about the role psychological factors play in how people experience pain has grown more widespread with the general shift away from the dualist view of the mind and body toward the more integrated biopsychosocial model. Chronic nonspecific low back pain “should not been considered as a homogenous condition meaning all cases are identical,” researchers in one review of the research on exercise cautioned.
A new understanding of pain called “central sensitization” is also gaining traction. The basic idea is that in some people who have ongoing pain, there are changes that occur between the body and brain that heighten pain sensitivity — to the point where even things that normally don’t hurt are perceived as painful. That means some people with chronic low back pain may actually be suffering from malfunctioning pain signals.
Enter alternative therapies for chronic back pain
Despite the clear risks, doctors have continued to prescribe painkillers, and perform surgeries and injections, sometimes to patients who won’t take no for answer or who can’t afford to try alternatives (which usually aren’t covered by insurance plans).
Slowly, though, the tide is shifting.
Medical societies and public health agencies are now advising doctors to try less invasive options and even alternative therapies such as acupuncture before considering opioids or surgery.
Most recently, in February 2017, the American College of Physicians advised doctors and patients try “non-drug therapies” such as exercise, acupuncture, tai chi, yoga, and even chiropractics, and avoid prescription drugs or surgical options wherever possible. (If the non-drug therapies fail, they recommended nonsteroidal anti-inflammatory drugs as a first-line therapy, or tramadol or duloxetine only as a second-line therapy.) In March 2016, the Centers for Disease Control and Prevention also came out with new guidelines urging health care providers to turn to non-drug options and non-opioid painkillers before considering opioids.
At the same time, research has mounted suggesting active therapies (exercise programs, yoga, tai chi) can really help people work through back pain, and alternative approaches (massage, spinal manipulation) can be effective, too — with the caveat that they’re often no panacea and the effects tend to be short-lived and moderate.
But most of the alternatives also carry little or no harm (except to patients’ pocketbooks) — which makes them all the more appealing amid the historic drug crisis.
“We have a slew of modalities and procedures that the American College of Physicians cannot endorse — such as opioids, fusion surgery, such as injections,” Ramin said, because there’s now so much evidence of ineffectiveness or harm. “So all those things are off the table, and now they are looking for things they can endorse that will not cause harm.”

You Might Also Like:


Moving is probably the most important thing you can do for back pain
When back pain strikes, your first instinct may be to avoid physical activity and retreat to the couch until the pain subsides.
But doctors now think that in most cases, this is probably the worst thing you can do. Studies comparing exercise to no exercise for chronic low back pain are consistently clear: Physical activity can help relieve pain, while being inactive can delay a person’s recovery.
Exercise is helpful for a number of reasons: It can increase muscle strength, which can help support the spine; It can improve flexibility and range of motion in the back, which can help people’s functional movement and get them back to their normal living; it can boost blood flow to the soft tissues in the back, which promotes healing and reduces stiffness. These are just a few reasons why researchers who study back pain suggest opting for exercise before some of the passive therapies like acupuncture or massage (we’ll describe those later).
Researchers in this 2016 review of the research on exercise for chronic nonspecific low back pain summarized exercise’s range of benefits, including these pretty amazing findings:
- “Aerobic exercise for 20 min on a cycle ergometer at 70% peak oxygen uptake reduced the pain perception for more than 30 min for patients with [chronic low back pain].”
- “Improving the flexibility of the lumbar spine and hamstrings can significantly reduce [chronic low back pain] by 18.5%–58%.”
- “Core stabilization programs have been shown to significantly reduce [chronic low back pain] by 39%–76.8%, and a muscular strength program significantly reduced [back pain] by 61.6%.”
Those researchers suggested that a combination of exercises — strength training, aerobic exercise, flexibility training — may be most helpful to patients, and that there seemed to be no clear winners among the different approaches but that each had its own benefits.
“My general take,” Chou said, “is that all [exercise types] seem to work.” If people find a program that makes them feel better, he added, they’ll probably see benefits not only with their back but with their overall health and sleep patterns, too.
To be clear, exercise doesn’t always help with those short-lived acute episodes. But if you have chronic back pain, you’ll want to find ways to work through the discomfort and keep active. Next, we’ll turn to some more specific exercises that are popular (and well studied) for back pain.
Yoga, Pilates, and tai chi seem to help — but it’s not clear that they’re any better than other exercise
There’s lots of research on back pain and yoga. Not all of it is high-quality, but taken together, the evidence pretty uniformly suggests yoga can both decrease pain and improve back-related function. (You can read more about yoga’s health benefits — and the difficulties of studying the practice — in this Show Me the Evidence.)
The most recent Cochrane systematic review on yoga and chronic low back pain, published in 2017, sums up the results of the best available studies, which mostly focused on the Iyengar, Hatha, or Viniyoga forms of yoga:
So again, this isn’t an end-all treatment — but the evidence we have points in the direction of a benefit.
Importantly, the review authors also noted that it’s not clear whether yoga is better than other exercises, since there were few head-to-head comparisons tracking yoga against other kinds of workouts.
As for tai chi and Pilates, the Agency for Healthcare Research and Quality (AHRQ), a federal agency that crunches the best available data on the effectiveness of health care interventions, recently published a comprehensive 800-page systematic review of research on noninvasive treatments for low back pain, including these two kinds of exercises. It found tai chi seemed to reduce chronic back pain and help people return to their daily activities when compared with no exercise, and that it was more effective in alleviating pain than backward walking or jogging but not necessarily better than swimming.
For Pilates, the evidence was a little more mixed: It was associated with small or no effects on pain and no effects on function compared with other types of exercise. Again, though, pretty much every back expert I spoke to said any exercise is better than no exercise, so if Pilates is something you enjoy, do it.
Try to find a “back whisperer,” or try these three exercises from one
Ramin, the journalist and author of Crooked, makes a compelling argument for seeking out a specialist who deeply understands the back to tailor an exercise program that targets your specific pain.
These “back whisperers” come from many different backgrounds: doctors of physical therapy with an orthopedic clinical specialist certification, personal trainers with a degree in exercise science, physical therapists.
“They are able to observe how you walk and sit and stand, and grasp what your posture and gait say about your muscles, tendons, and ligaments,” she writes in Crooked. “Generally, they focus on functional training, prescribing exercise regimens that are ‘non-pain-contingent’ (you don’t stop when it hurts, sorry), ‘quantitative’ (you will not be allowed to quit until you hit your ‘number’), and ‘high-dose’ (you will do this routine on a schedule rather than when the spirit moves you).”
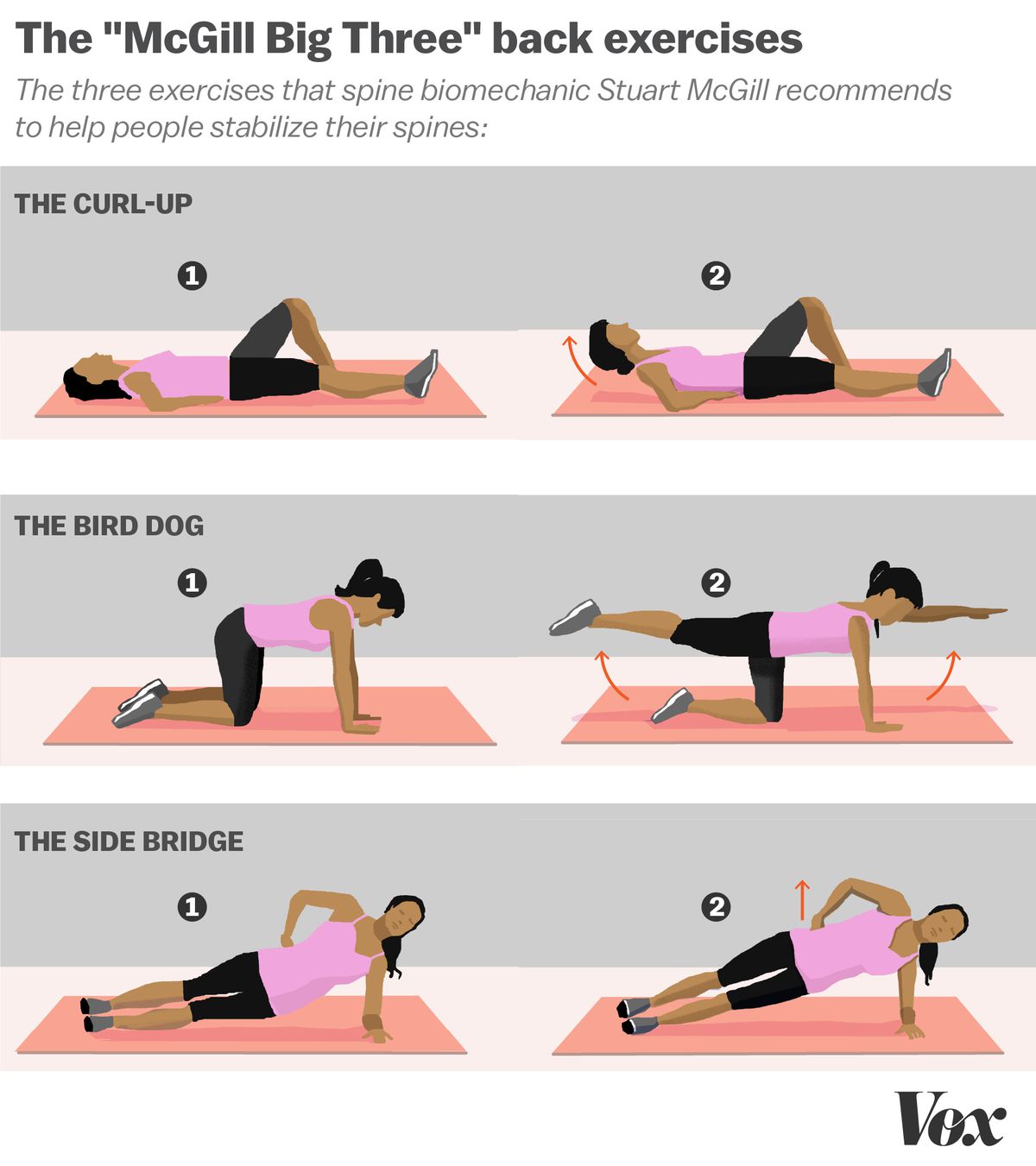
One renowned “back whisperer” is spine biomechanics professor Stuart McGill, of the University of Waterloo in Canada, who has treated everyone from Olympic athletes to professional football players. He spends several hours watching his patients move, and identifies the specific motions, postures, and loads that trigger their back pain. He then tailors exercise programs that build a foundation for pain-free activity, so that those triggers no longer result in pain. (He’s also written a popular book, Back Mechanic, which walks readers through his process — an approach based on decades of research at his spine biomechanics lab and clinic at the University of Waterloo.)
McGill has a set of spine-stabilizing exercises — the McGill Big Three, which Ramin does daily — based on research in his lab that are targeted at people with chronic back pain.
It can be difficult to find someone with the expertise of a back whisperer like McGill, and their time can also be costly. There’s also no study that brings together research on these folks, but if you can find a good one who works for you, your back pain could be improved.
We’re learning how much back pain is mental, and that mind-body approaches can help
So where does physical therapy — usually a combination of guided exercises, mobilization, superficial heat or cold, and health advice — fit into the back pain treatment picture?
In AHRQ’s read of the evidence, it didn’t seem to work better than simple advice to remain active when it came to reducing pain and improving function. (The researchers I talked to said this lack of effect may be because of the variability in physiotherapy approaches and programs, and the difficulty in coming to clear conclusions about the variety of programs on offer.)
Nowadays, though, there are also several different kinds of physical therapies that also integrate psychotherapy or cognitive behavioral therapy, often called multidisciplinary rehabilitation.
Multidisciplinary rehab takes the “biopsychosocial” view of back pain — again, that the pain arises from the interplay of physical, psychological, and social factors. It can of course be tricky to disentangle whether mood disorders like anxiety or depression contribute to people’s pain, or whether they arise out of the pain, but either way, the biopsychosocial model views the physical as only one part of the equation. So these practitioners deal with what’s going on inside the head as part of their back pain therapy — helping patients get treatment for their depression or anxiety, or guiding them through cognitive behavioral therapy to improve their coping skills.
Perhaps not surprisingly, multidisciplinary therapy appears to work slightly better than physical therapy alone for chronic back pain in both the short and long term. Patients who get these more holistic treatments are also more likely to return to work.
Spinal manipulation by chiropractors works about as well as exercise or over-the-counter drugs — with some big caveats
Passive therapies can also play a role in helping people manage back pain, though there’s no silver bullet among them, and their effects also tend to be modest and short-lived. (Again, active approaches to managing back pain should be your first stop.) The research base for these alternative therapies is also generally weak: There’s a lot of variability among the practice styles and programs on offer, even within one category of treatment like massage. It can be difficult to blind the patients to the treatment they are receiving, and the people who seek out particular therapies — acupuncture, massage — are probably more amenable to them, which may bias the results. With that said, here’s what we know.
Spinal manipulation, the cranking and tweaking on offer when you visit a traditional chiropractor, is among the most popular approaches to back pain. Practitioners lay their hands on the patient and move their joints to or beyond their range of motion — a technique that’s often accompanied by a pop or crack.
There is some evidence the approach can help people with chronic back pain — but not any more than over-the-counter painkillers or exercise, and you need to take precautions when seeking out a chiropractor.
First, a quick look at the evidence. There are two recent Cochrane reviews on spinal manipulation for low back pain: one focused on people with acute (again, episodic/short duration) pain and the other on chronic pain. The 2011 review on chronic low back pain found that spinal manipulation had small, short-term effects on reducing pain and improving the patient’s functional status — but this effect was about the same as other common therapies for chronic low back pain, such as exercise. That review was published in 2011; UpToDate reviewed the randomized trials that have come out since — and also found that spinal manipulation delivered modest, short-term benefits for chronic back pain sufferers.
The Cochrane review on acute pain found that spinal manipulation worked no better than placebo. So people with a short episode of back pain should probably not bother seeing a chiropractor.
“Based on the evidence,” University of Amsterdam assistant professor Sidney Rubinstein, who is the lead author on the Cochrane reviews, told me, “it would appear [spinal manipulation] works as well as other accepted conservative therapies for chronic low back pain, such as non-prescription medication or exercise, but less well for patients with acute low back pain.”
As a chiropractor himself, he had some advice for patients: They should avoid chiropractors who routinely make X-rays or do advanced diagnostics for low back pain because this adds nothing to the clinical picture, particularly in the case of nonspecific low back pain. Patients should also beware chiropractors who put them on extended programs of care.
“Patients who respond to chiropractic care traditionally respond rather quickly,” he said. “My advice is those patients who have not responded to a short course of chiropractic care or manipulation should consider another type of therapy.”
While the risks of serious side effects from spinal manipulation for back pain are rare — about one in 10 million — the risks associated with chiropractic therapy for neck pain tend to be slightly higher: 1.46 strokes for every million neck adjustments.
The issue is the vertebral artery, which travels from the neck down through the vertebrae. Manipulating the neck can put patients at a higher risk of arterial problems, including stroke or vertebral artery dissection, or the tearing of the vertebral artery (though Rubinstein noted that people in the initial stages of stroke or dissection may also seek out care for their symptoms, such as neck pain, which makes it difficult to untangle how many of health emergencies are brought on by the adjustments).
The results on massage are mixed — but it’s also pretty harmless
In general, massage therapists work by manipulating the muscle and soft tissue of the back and body. There are many, many different styles of massage: Swedish, deep tissue, sport, myofascial release, Thai, the list goes on. Massages also vary in how long they last, how much pressure is used, and how frequent sessions are, which makes the evidence for massage pretty difficult to interpret.
But there’s good news here: Massage is pretty harmless, and the researchers who study back pain say the approach makes sense from a pain relief perspective. So it may be worth trying.
According to AHRQ, for subacute (lasting between seven and 12 weeks) and chronic low back pain, massage seems to improve symptoms and function in the short term (i.e., one week) — but there’s no evidence that it leads to any long-term change. At best, you’ll get a bit of immediate relief, but nothing lasting.
The Cochrane systematic review on massage for low back pain looked at 25 trials on massage and, like AHRQ, found short-term improvements in pain and function for both subacute and chronic low back pain but a very mixed evidence base.
Acupuncture seems to help too — sort of — though it’s more controversial
One of the oldest approaches to back pain is acupuncture, a core part of traditional Chinese medicine. The philosophical underpinning of acupuncture is that disease or pain in the body is the result of imbalances between the body’s “yin and yang forces.” “Vital energy circulates throughout the body along the so-called meridians, which have either Yin or Yang characteristics,” the Cochrane authors explain. Using needles to stimulate the parts of the body that are located on these meridians can modulate pain or reverse disease, practitioners claim.
A 2005 Cochrane review looked at the evidence for acupuncture and low back pain and came to a few useful conclusions: There was “insufficient evidence” to make any recommendations about acupuncture for acute low back pain — so it may or may not help people. For chronic pain, acupuncture seemed to offer more pain relief when compared with no treatment or sham acupuncture (when practitioners use needles that don’t actually penetrate the skin). The needling also improved function in the short-term when compared with no treatment for chronic pain sufferers. But acupuncture was not more effective than other treatments.
UpToDate looked at more recent research and noted that the studies on acute pain were still limited, and that evidence for acupuncture’s effects on chronic pain is somewhat conflicting. The review also noted it was unclear whether acupuncture’s benefit lies in the needling, or in the placebo effect.
The author of the Cochrane review, Andrea Furlan, pointed to a more recent randomized trial, which came out in 2009 after her review was published: It also found that acupuncture seemed to reduce chronic low back pain — but it didn’t seem to matter where the needles were placed, raising questions about the meridian philosophy guiding the practice.
This is what makes acupuncture controversial. Science suggests it might work — but the squishiness of the findings, combined with the lack of scientific underpinning in acupuncture’s philosophy, leaves room for interpretation. And evidence-based medicine thinkers and skeptics view the results of studies as suggestive of nothing more than acupuncture’s potent placebo effect.
Researchers have found that the more dramatic the medical intervention, the stronger the placebo effect. And getting poked all over the body by needles is a pretty dramatic intervention. (See this classic study comparing water injections with sugar pills for migraines, as well as Vox’s placebo explainer by Brian Resnick.) That’s not to mention you can never run a double-blind placebo — the gold standard in health research — on acupuncture, since that would involve both practitioners and patients not knowing (or being blinded to) what treatment they are giving and receiving.
We need make our default choices more back- (and health-) friendly
There’s a pretty simple adage public health officials stick to: Make it easy for people to stay healthy, and make it hard for them to get sick.
When it comes to back pain in America, we make it easy for people to get sick and hard for them to stay healthy.
There’s a complete disconnect between what insurance providers will cover for people and what actually helps their back pain. It’s still much easier to get your opioids or back surgery paid for by your insurance provider than to get a massage or exercise program reimbursed.
More states need to move in the direction of places like Oregon, where insurance payers are making the default options for people with back pain healthier by expanding access to, and coverage for, non-drug options.
For example, the Oregon Health Plan (the state’s version of Medicaid, federally funded health insurance for the poor) has ensured that alternatives like acupuncture and physical therapy are covered. It’s also expanded access to treatment for the behavioral health factors that are associated with back pain (such as depression and anxiety) by paying primary care clinics extra to be able to hire behavioral health specialists and meet patients who may not have had access to those services. Finally, it’s opened non-medication pain clinics, where people with low back pain can get a range of treatments as well as help to taper off their opioid prescriptions.
Amit Shah, the chief medical officer at CareOregon (one of the insurance companies administering the Oregon Health Plan), said they decided to move in this direction in the face of the mounting evidence of the harm opioids were causing. “Chronic lower back pain is very prevalent, and we know some people with chronic lower back pain have used opioids for it,” he said. “There’s been a lot of evidence and studies about how opioids are not necessarily the most effective approach, while other medical interventions are effective.”
This knowledge, along with “the continual realization that patients deserve more than a prescription that doesn’t necessarily work,” Shah said, pushed Oregon to experiment with a new benefit structure that might actually help people. “We’re trying to expand the options instead of limiting choice only to opioids.”
Officials in Oregon haven’t yet determined the cost of this new scheme, but opioid prescriptions are already down. Shah also said he’s confident that the measures are bound to reduce the cost burden overall, since alleviating pain can help people can get back to work and bring down the numbers of opioid deaths. If only other states would follow Oregon and take back pain this seriously.
Addendum: America’s most famous back guru
No back pain article would be complete without a mention of the late John Sarno, an NYU professor of rehabilitation medicine and probably America’s best-known back guru. He believed there is an emotional basis for all chronic back pain.
More specifically, he thought that the brain distracts us from experiencing negative emotions by creating pain. We may not want to accept the uncomfortable truths that we are angry with our children, or that we hate our job, so instead of thinking those thoughts, we focus on the pain.
Back pain researchers and doctors generally still don’t find Sarno’s theories entirely convincing — particularly his one-size-fits-all diagnosis — and I’ve written about why at length here. But Sarno got some things right. As I’ve mentioned, it’s now mainstream to view chronic back pain as a “biopsychosocial” condition, and “central sensitization” is also gaining traction. Both ideas suggest it’s not just what’s going on in your body and back that matters for your pain.
That means he was also ahead of his time when it came to treatment. “What [Sarno] recommended as treatment was essentially cognitive behavioral therapy — elimination of fear avoidant behavior and catastrophizing — before anyone had ever heard of it,” Ramin said, “and it’s exactly what is being used now to treat patients with central sensitization.”
*A note on the methods for this installment of Show Me the Evidence
There’s a mountain of research on low back pain. (Entering the term in the PubMed search engine turned up more than 31,000 results.) So I zeroed in on the highest-quality evidence: systematic reviews. These are syntheses of the research evidence that bring together all the highest-quality studies to come to more fully supported conclusions.
I found the Agency for Healthcare Research and Quality (AHRQ), a federal agency that crunches the best available data on the effectiveness of health care interventions and had recently (February 2016) published a comprehensive 800-page systematic review of research on noninvasive treatments for low back pain. The AHRQ review covered 156 of the best back pain studies from 2008 to April 2015. I then searched for low back pain–related systematic reviews on PubMed Health, the government search engine that specializes in systematic reviews and meta-analyses, to cover the recent period left out of the AHRQ review (from May 2015 to the present, July 2017).
To make sure I wasn’t missing anything, I consulted the chronic and acute low back pain articles on UpToDate, (a service that synthesizes the best available research for clinicians), the Cochrane Library of systematic reviews, and guidelines.gov, and sometimes followed the footnotes in these reviews to other studies. Ramin’s book Crooked was also an excellent source for thinking on back pain. Finally, I conducted interviews with nine back pain doctors and researchers, including authors of many of the systematic reviews referenced here.
Correction: A previous version of this article referred to John Sarno’s medical specialty as psychiatry. Instead, it was rehabilitation medicine.
This article was originally published here